
First Some Logistics
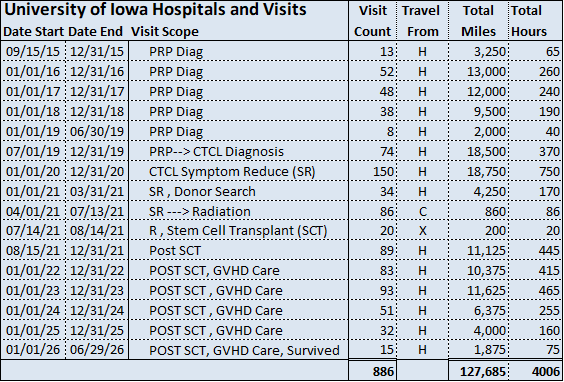
A Reasonable Estimate: Appendix A, Chart 1

My deadline approaches. My wife has come up with a reminder. I am to play or think of the line from the song: “Midnight at the oasis…sing your camel to bed.” The next essay in Two Years a Vampire will focus on “Who was the starting pitcher?” I made that analogy in the essay “What Brought Me Here.”
Preparatory to delving into all that, I have started to collect data that is related to my entire sequence of clinic visits, the hospital stay, and conversations with my healthcare experts. The first medical summary download for a small portion of the timeframe 09/15/2015 to 12/31/2015 is a .pdf document some 250 pages long.
My plan is to create a table of contents and an index for the entire set. This is a project.
Meanwhile, I came up with this idea: why not create a table that shows meaningful date ranges of my visits and the scope or stage of treatment. The University Hospitals and Clinics uses the MyChart application. I can use it to tell me the number of visits in a timespan. The table above is the result. I added travel distance—250 miles round trip from our home to Iowa City, for example, and a rule of thumb trip hours estimate.
Therefore, H = Home; C = Coralville, IA, near Iowa City, and X = Hospital. I have hidden the column that adjusts for situations where one trip to Iowa City results in two visits. For example, once the diagnosis of cutaneous T-cell Lymphoma arrived (CTCL), I then visited both the stem cell transplant oncologist and a specialist in diseases and cancers that impact the skin. One trip, two clinics at the U of I. By “Hours” I mean on-the-road road time, not time at the clinic visits. Could add that.
I can try this lame pun: when the cancer illness was in full flower, my skin was not “cute”-aneous.
The table is reasonably accurate. I do not account for the brief period in which I stayed at my sister's house near the hospital. One procedure required that I travel to Iowa City every two week for two-day’s of the same recommended and often therapeutic procedure.
Staying with my sister and her family was very helpful and enjoyable, and I am grateful for that. Covid quickly put an end to that convenience. CTCL caused my skin to drastically loose its ability to ward off infections, and my body and mind were under a high degree of stress. (I am acknowledging that COVID is not caught via the skin vector.)
PRP? At the top of the table I have listed under scope something named “PRP Diag.” What is that? When I showed up at the Dermatology Clinic in 2015, the staff had already reviewed my charts and the pathologists analysis of the skin punch biopsies. The biopsies were taken at a local dermatologist’s clinic. The constellation of symptoms indicated PRP—Pityriasis Rubra Pilaris. A deep delve into that awaits. I sum it up this way: no one wants to be told they have cancer when they do not. The full clinical examinations and pathological tests had not provided the criteria for a solid diagnosis for CTCL in 2015.
I am satisfied that my expert dermatology team arrived with all due diligence and care at the diagnosis of PRP in 2015. Best fit.
One last: there is a six month period in which I attended just eight clinical visits. Had I been following the suggested regime, the frequency would have been at least twice that.
I drove most of those miles and hours by myself. Sometimes I took US Highway 6, the older version on which Jack Kerouac and Neal Cassidy as Dean Moriarty raced through the state of Iowa on two wheels, as it were.
Well, cancer nearly had me beat in that timeframe. The diagnosis had not yet arrived, although it was imminent. I had not entirely given up and refused to think too seriously about the alternative. Not giving up is my default mode.
I am grateful it is so. We can wait on the definition of “GVHD.”
Midnight at the Oasis is playing.